
Zinc Testing: Sand Castles in the Air (Part 7)
Why Blood Tests Capture Less Than 0.1% of Your Zinc—and What That Really Means for Diagnosis

Disclosure: As a co-owner of Aurmina, one of the products discussed below, I have a financial interest in it. This article is for educational purposes only and reflects my personal opinions and experiences as a clinician. It is not intended as medical advice, and any health-related decisions should be made in consultation with a qualified healthcare provider. Products mentioned are not intended to diagnose, treat, cure, or prevent any disease.
Dear readers,
If you’ve been following along with this series—from Ketamine and the Mineral Bridge , where we explored zinc’s foundational role in bridging neurological and metabolic pathways, to The Hippocampus Under Siege, examining how zinc deficiencies exacerbate brain vulnerabilities; NMDA Protection, AMPA Trouble, delving into zinc’s dual modulation of glutamate receptors; The Zinc Threshold We Missed, highlighting overlooked tipping points in zinc homeostasis; Zinc’s Double-Edged Sword, balancing its protective and potentially toxic effects; and the first article in the series, The Zinc Paradox, unpacking the counterintuitive ways zinc influences health—then you know we’ve been building a nuanced picture of this essential mineral. Zinc isn’t just a supplement; it’s a linchpin in our body’s intricate web of enzymatic, neurological, and immunological functions.
In this seventh installment, we’re turning our attention to the tools we use to measure zinc status. As a Family Nurse Practitioner (FNP-C) with years of clinical experience, I’ve ordered my share of zinc tests and interpreted results to guide patient care. But the more I dig into the science, the more I question the foundation of these practices. Today, we’ll discuss the pros and cons of common zinc testing methods, with a critical eye on their severe limitations. We’ll see how relying on them without context is like building sand castles in the air—impressive at a glance, but fragile and disconnected from the deeper realities of mineral dynamics. And we’ll explore how emerging insights, including those related to ionic sulfated products like Adya Clarity and Aurmina, could potentially shift our approach.
The Limitations of Blood-Based Zinc Testing: A Tiny Window into a Vast Reservoir
Let’s start with the elephant in the room: Most clinical decisions about zinc supplementation or deficiency are based on blood tests—specifically serum/plasma or red blood cell (RBC) zinc levels. These are the go-to methods in conventional medicine, often ordered alongside routine labs. But here’s the stark reality: Less than 0.1% of the body’s total zinc is actually in the blood [1,2]. The vast majority—around 50-60% in skeletal muscle, 30% in bone, and the rest scattered in skin, liver, and other tissues—remains invisible to these tests [3].
Serum/Plasma Zinc: The Quick but Flawed Snapshot
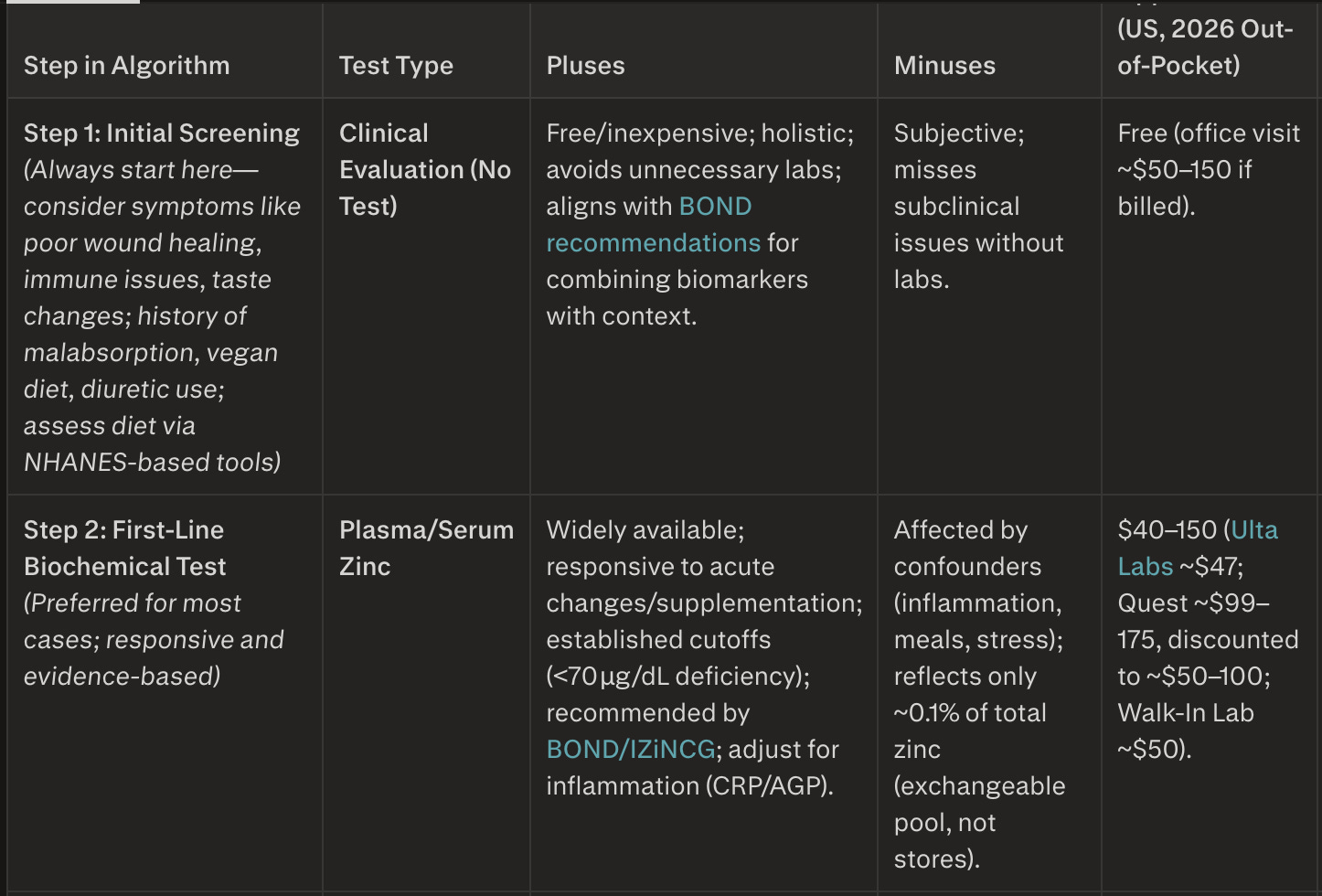
Pros: Widely available, affordable (around $40-100), and responsive to acute changes like supplementation or severe deficiency. It’s the standard recommended by expert panels like the Biomarkers of Nutrition for Development (BOND) Zinc Expert Panel [4].
Cons: Highly influenced by factors like inflammation, recent meals, stress, or even time of day. It only reflects the small, rapidly exchangeable pool of zinc, not total body stores. Without adjustments (e.g., for C-reactive protein to account for inflammation), results can mislead. And yet, clinicians often base dosing on this alone, ignoring that it captures such a minuscule fraction of zinc.
RBC Zinc: The “Intracellular” Myth in Functional Circles
In functional and integrative medicine, RBC zinc is sometimes touted as a “longer-term” or “intracellular” measure, supposedly less swayed by short-term fluctuations. But as we’ve discussed in prior parts of this series (e.g., the thresholds in [The Zinc Threshold We Missed]), this view isn’t strongly supported by rigorous reviews.
Pros: Measures zinc inside red blood cells (where 75-80% of blood zinc resides), potentially offering insight into chronic status.
Cons: Depletion and supplementation studies show it doesn’t consistently respond to zinc changes [4,5]. The BOND panel classifies it as “non-useful,” and major labs like Mayo Clinic have discontinued it (in 2019), citing no advantages over serum [4]. Promoting it as superior is often anecdotal, not evidence-based—echoing the paradoxes we unpacked in [The Zinc Paradox].
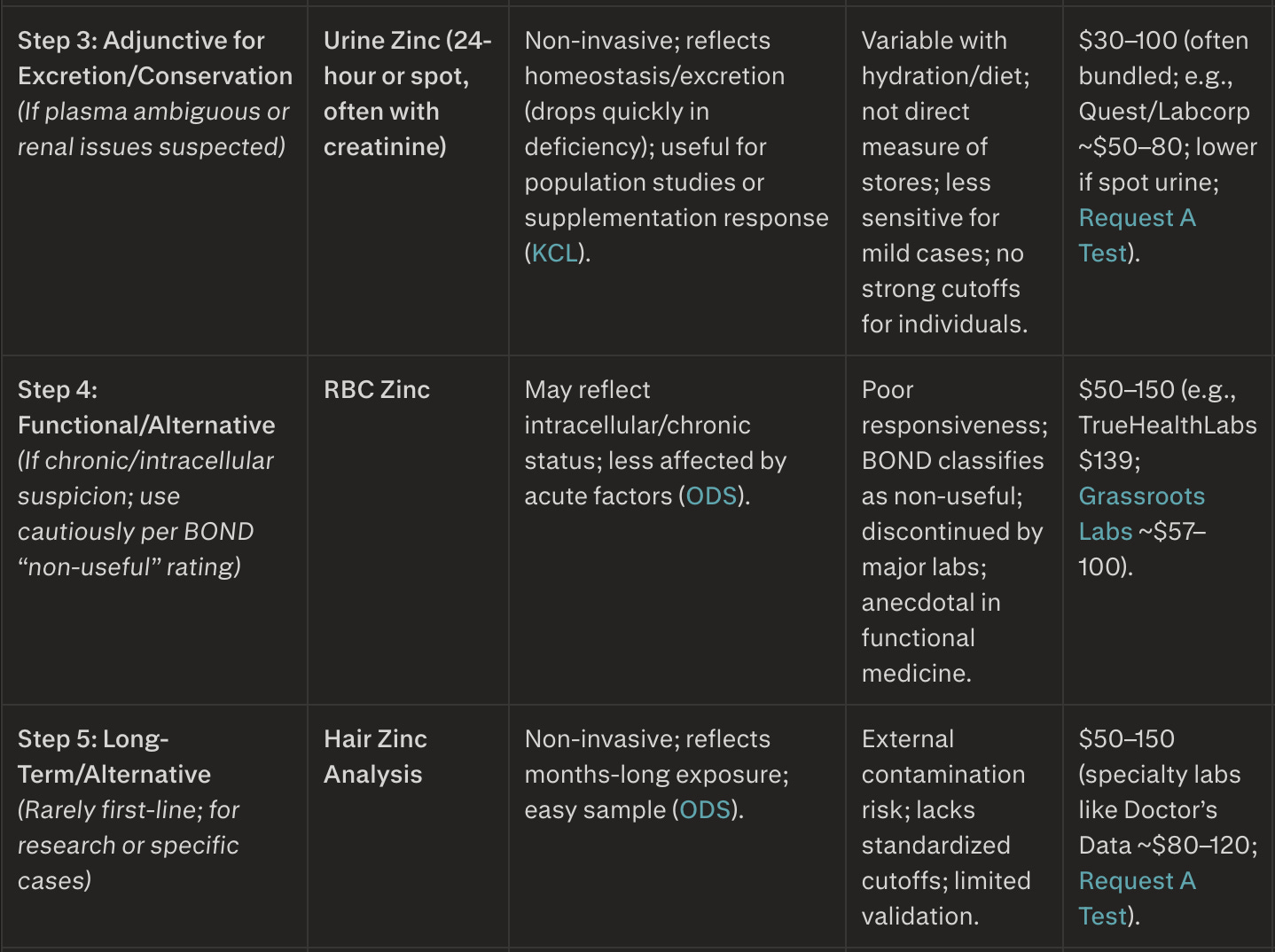
Other tests like urine (reflects excretion dynamics but not stores) or hair (longer-term but prone to contamination) have their niches, but none escape the core issue: They’re indirect proxies, built on dated frameworks that don’t fully account for modern mineral science.
That said, more comprehensive urinary profiling offers promising potential for real-time insights. Over the past four months, as the Principal Investigator in an IRB-approved clinical study, I’ve been exploring this shift using Adya Clarity as the intervention. We’re measuring changes in precipitation of toxic metals and shifts in 24-hour urinary excretion of minerals, trace minerals, and rare earth elements via the Urine Toxic and Essential Elements test from Doctor’s Data. This panel—capturing both toxic burdens and a broad spectrum of essential/nutrient dynamics (including zinc excretion)—has proven remarkably valuable in my practice, providing a dynamic, functional view of mineral status that feels far more reflective of real-time zinc utilization than static blood snapshots alone. Early observations suggest these ionic sulfated coherencing therapies may enhance the body’s innate capacity to extract, organize, and utilize minerals already present in the diet—potentially elevating effective systemic zinc availability without relying on additional trace mineral supplementation. While the study is ongoing and results preliminary, this approach could prove integral to redefining minimal zinc thresholds and moving toward a more accurate, utilization-focused paradigm for mineral assessment. These are emerging observations and have not been evaluated by the FDA; the products discussed are not intended to diagnose, treat, cure, or prevent any disease.
Dated Foundations: Ignoring Trace, Ultra-Trace, and Rare Earth Minerals
The U.S. Recommended Dietary Allowance (RDA) for zinc—11 mg/day for men, 8 mg/day for women—stems from 2001 guidelines based on balance studies from the 1980s and ‘90s. Testing cutoffs (e.g., <70 μg/dL for serum deficiency) draw from even earlier work, like Prasad’s 1960s discoveries. These are solid starts, but they predate our understanding of how zinc interacts with trace (e.g., selenium, molybdenum), ultra-trace (e.g., boron, vanadium), and rare earth elements (e.g., lanthanum, cerium). These minerals aren’t just background players; they may modulate enzymatic activity, absorption, and homeostasis in ways that amplify or mitigate zinc’s effects—think of the double-edged sword we discussed in part 5 [6,7].Without incorporating these insights, our recommendations feel like sand castles: Precarious structures built on shifting sands of incomplete data. For instance, if a patient’s diet is rich in phytates (zinc binders) but also in rare earths from soil-grown foods, their true zinc utilization might be far higher than a blood test suggests. We’re missing the forest for the trees.
Shifting the Paradigm: Ionic Sulfated Products and Coherent Water
This is where the conversation gets exciting—and ties back to the mineral bridges we built in part 1. Products like Adya Clarity and Aurmina aren’t just water purifiers; they may represent emerging approaches to mineral bioavailability. Derived from volcanic minerals (black mica or biotite), these ionic sulfated solutions are thought to organize water into coherent, structured forms—hexagonal clusters that potentially enhance cellular hydration and enzymatic function. These statements have not been evaluated by the FDA. These products are not intended to diagnose, treat, cure, or prevent any disease.
How They May Work: Through ion exchange, they reduce contaminants (up to 250+, including heavy metals and fluoride) while providing trace minerals in bioavailable forms. More crucially, their sulfated ions may support enzymes, potentially enabling better absorption and utilization of minerals already in your diet. This isn’t about mega-dosing; it’s about efficiency, echoing the NMDA/AMPA balances in part 3.
My colleague Dr. Pierre Kory has been a pioneer here, exploring coherent water in his Substack Pierre Kory’s Medical Musings. In posts like “Water Quality, Structure, and the Biology of Performance” and “The Inner Life of Water: Memory, Structure, and Consciousness”, he details how sulfated mineral coherent (SMC) water—potentially restored by products like Aurmina—may support metabolic stability and biological legibility. Unlike “dead” purified water, coherent water may foster structured domains that enhance enzymatic activity, potentially unlocking zinc and other minerals from food sources we already consume. This aligns with the hippocampus protections in part 2, where structured hydration could potentially mitigate siege-like stressors.In essence, these products may not just address testing—they could potentially transform how we access it, rendering outdated metrics even more obsolete.
Moving Forward: Beyond Sand Castles
As we wrap this series, remember: Best practice for zinc assessment integrates symptoms (e.g., poor wound healing, immune issues, neuro-cognitive impairment), history, dietary evaluation, and plasma zinc (inflammation-adjusted). RBC zinc? It’s intriguing in functional contexts but lacks robust backing [4,5]. By considering coherent water and ionic sulfates, we may shift from reactive supplementation to proactive utilization—building on solid ground.
Note: The views expressed here are my own and based on available research. Always verify claims with independent sources and consult professionals for personalized advice. As always, consult your provider before changes.
In health,
Scott Marsland, FNP-C
@RhusToxidendronon X
Lightning Bug Substack
References
King JC, Shames DM, Woodhouse LR. Serum zinc concentration as an indicator of population zinc status. Food and Nutrition Bulletin. 2007;28(3_suppl):S403-S429. doi:10.1177/15648265070283S303
NIH Office of Dietary Supplements. Zinc: Fact Sheet for Health Professionals. Updated 2024. Available at: https://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/
Al-Jawadi A, et al. Zinc Deficiency in Critically Ill Patients: Impact on Clinical Outcome. Cureus. 2024;16(3):e56789. doi:10.7759/cureus.56789
King JC, et al. Biomarkers of Nutrition for Development (BOND)-Zinc Review. The Journal of Nutrition. 2016;146(4):858S-885S. doi:10.3945/jn.115.220079 (PMC4807640)
Wessells KR, et al. Existing knowledge on Zn status biomarkers (1963–2021) with a systematic review and meta-analysis. Frontiers in Nutrition. 2023;9:1057156. doi:10.3389/fnut.2022.1057156
Mertz W. The essential trace elements. Science. 1981;213(4514):1332-1338. doi:10.1126/science.7022654 (Note: Classic foundational review on trace element interactions, including zinc.)
Sandstead HH. Interactions of zinc with other essential trace elements. American Journal of Clinical Nutrition. 1985;41(5):1029-1034. doi:10.1093/ajcn/41.5.1029 (Updated discussions in later reviews build on this.)
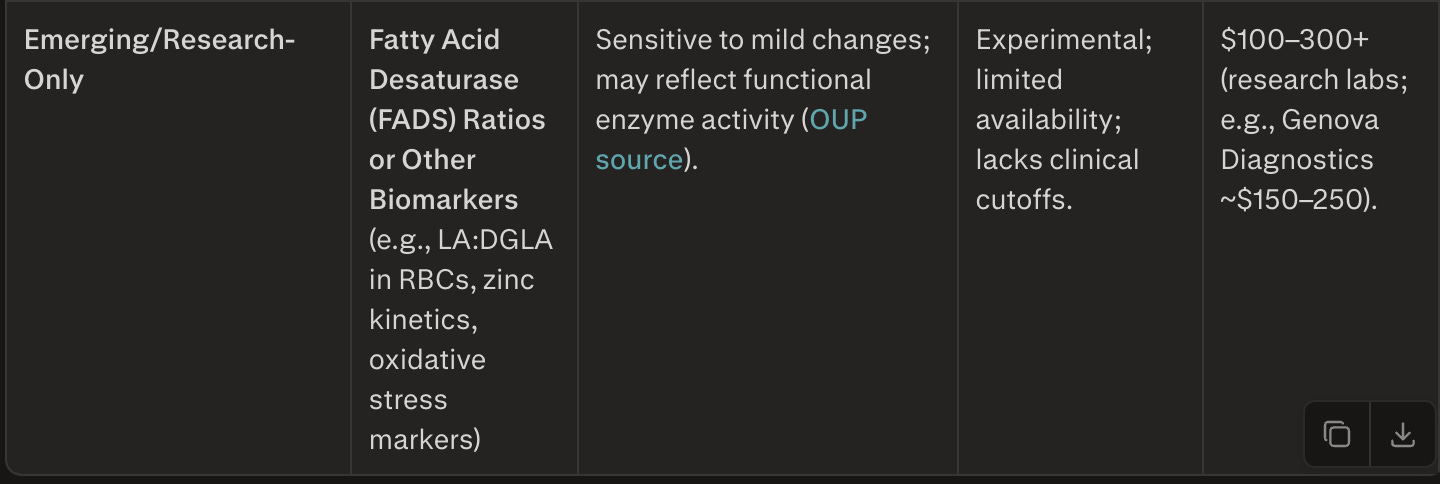
Clinician's Algorithm Table for Zinc Testing
Notes for Clinicians
Escalation logic:
If Step 1 or 2 confirms deficiency (e.g., low plasma zinc), supplement 15 – 30 mg/day elemental zinc for 3 – 6 months, then retest. Escalate only for discordant results or persistent symptoms.Best practice:
Integrate labs with clinical findings and diet history — avoid relying on single biomarkers.Cost notes:
Based on 2026 pricing (Quest, Labcorp, Ulta, Walk‑In). Direct‑to‑consumer services often cheapest.Billing:
Most basic tests covered with ICD‑10 E61.1 (“Zinc deficiency”). Functional/integrative tests typically self‑pay.
##Zinc Dosing Poll—Your Turn!
Come for the science, stay for the stories.
The My Vietnam series and other personal reflections live in the opt-in Personal Insights section—toggle it on in your account settings if they resonate.
Dear Cathryn and Bill,
Thank you both for your thoughtful comments and for engaging so deeply with the series—it's great to see readers connecting the dots and sharing their experiences.
Regarding the OligoScan (also known as Oligo/Check in some regions): Yes, I'm familiar with it, in part from researching for this seven part series, although I haven't used it. For the benefit of other readers: OligoScan is a non-invasive handheld device that uses spectrophotometry (measuring light absorption/reflection through the skin, typically on the palm) to estimate tissue levels of minerals, trace elements, vitamins, oxidative stress, and heavy metals in real time. Practitioners often value it for providing quick "intracellular" or "tissue" insights without blood draws, urine collections, or hair samples, which can feel more direct than circulating levels in serum/plasma.
That said, my opinion on its accuracy and reliability is cautious, leaning towards skeptical, and aligns with the broader evidence landscape we've discussed in this series (e.g., the need for robust validation of any biomarker). Strengths noted by users and some practitioner reports include its convenience, speed, and potential to reflect longer-term tissue storage (rather than transient blood fluctuations). Some comparative studies cited by manufacturers or users suggest reasonable correlation with lab methods for certain elements in controlled settings.
Limitations and criticisms from skeptical reviews (e.g. discussions on platforms like ResearchGate) highlight a lack of strong, independent, peer-reviewed validation. Key concerns include:No large-scale, blinded studies comparing OligoScan results head-to-head with gold-standard lab methods (e.g., ICP-MS on tissue biopsies or validated blood/urine/hair panels) across diverse populations. Listen, I bristle at the demands for large-scale, blinded studies before mainstream practitioners will adopt ANY therapy or testing, BUT, we're talking about a testing method which will guide treatment. It's really important to note whether a test is validated or not.
Potential variability from factors like skin thickness, temperature, hydration, calibration drift, or operator technique—common with handheld spectrophotometric devices.
Claims of "intracellular" or "tissue" accuracy are appealing in functional/integrative contexts but aren't strongly supported by rigorous external evidence; the technology measures optical properties at the skin surface, and extrapolating to whole-body intracellular status requires more substantiation.
It's not classified as a diagnostic medical device in many regulatory frameworks (e.g., not FDA-cleared for quantitative mineral/heavy metal assessment), so results are often positioned as "functional insights" rather than definitive clinical values.
In short: OligoScan could maybe, possibly be a useful screening or monitoring tool in the hands of experienced practitioners who integrate it with symptoms, history, diet, and other labs (similar to how we use hair or spot urine tests). But like serum/RBC zinc (which we've critiqued for capturing only a tiny fraction of total body zinc), it shouldn't stand alone as the definitive measure of status—especially for guiding major interventions. If your OligoScan shows low cellular zinc and other imbalances, it's worth correlating with additional markers (e.g., plasma zinc with inflammation adjustment, 24-hour urine for excretion dynamics, or even the Doctor's Data panel I mentioned in the post) to build a fuller picture.
I'm open to learning more—have you found the OligoScan trends consistent over time in your own follow-ups, or correlated well with symptom improvements? Thanks again for sharing your journey, and best wishes as you address those dental factors and support your thyroid health.
Feel free to reply with more details if you'd like to discuss further—I'm here! Because I'm a real clinician who sees real patients, it may be a hot minute before I respond, but I'll try.
Warm regards,
Scott Marsland, FNP-C
Dear readers and fellow travelers in the zinc wilderness,
With this post—Part 7: Zinc Testing: Sand Castles in the Air?—we're reaching what feels like a natural pause in the Lightning Bug zinc series. We've journeyed from ketamine bridges and hippocampal sieges, through NMDA/AMPA balances, missed thresholds, double-edged swords, paradoxes, and now the shaky foundations of how we even measure zinc status.
For now, this marks the final installment... but only for now. My ongoing IRB-approved study (now four months in) with Adya Clarity and the Doctor's Data 24-hour Urine Toxic & Essential Elements test is generating intriguing preliminary data on real-time mineral dynamics, excretion shifts, and how ionic sulfated coherencing might unlock better utilization from the diet we already eat—no extra trace mineral megadosing required. As we analyze and extrapolate from those results over the coming months, I'll almost certainly return with updates, refinements, or even a "Part 8: Zinc Revisited" when the picture sharpens.
In the meantime, I'd love your input to see how this series has landed in real life. If you've been reading along, have you changed your approach to zinc assessment, supplementation, or testing? Noticed any shifts in symptoms, energy, mood, immunity, or other markers? What resonated most—or what questions remain?
To make it easy, I've created a quick reader survey: https://lightningbug.substack.com/i/188323692/zinc-dosing-pollyour-turn
It should take less than one minute, and your anonymous responses will help shape whatever comes next. (Substack surveys/polls are subscriber-only by default, but feel free to share thoughts in the comments too.)
Thank you for joining this exploration—your engagement has made it richer than I could have imagined. Let's keep the conversation going.
In health and curiosity,
Scott Marsland, FNP-C
@RhusToxidendron on X