
Soy un perdedor
Losing sports, a union drive, a pandemic and finding IVM

PAST
The West Hartford, CT of my boyhood had a well-developed soccer league. In Connecticut public schools, soccer had more sway than football. For three years I played right wing for a team called the Darts. Our uniforms consisted of green and white jerseys, with white shorts.
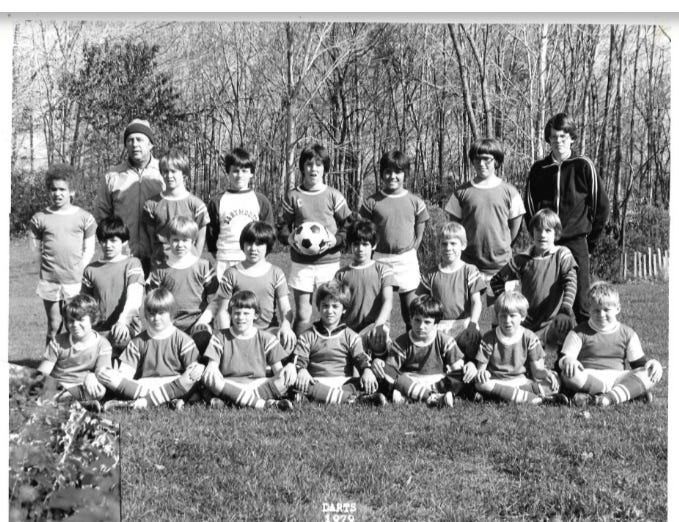
Our head coach was a chain smoking man who I only knew as Coach Miller. I also saw him at our house playing bridge with my parents and other adults. Our team had a few assistant coaches, including a tall, bespectacled, red-headed high school kid who would carpool with us to practice and games. There was a fullback named Tank who also sang in the church choir with me. That’s Tank bottom right in the photo, with me next to him. Timmy was the star center striker who was as fleet of foot as he was handsome.
I loved to play, but I was not very good. In fact, the best I could expect was to play one of four quarters in any given game—for three years. I never made a goal. If I assisted a goal it was by accident. If our team won any games, I don’t remember them. I was a lackluster player on a losing team. At the time, I simply accepted my experience. Kind of like a dog that’s missing one of its legs that doesn’t lay around feeling sorry for itself, and gets on with the business of life. It helped me get scrappy and it sure helped prepare me for life.
I would say my experience of being a loser on a losing team was a net positive. There were winning moments in the course of losing a game. I could take great pleasure in watching Tank bring the center of an opposing team to an abrupt stop with a slide and kick that sent the ball across the field into their goalie’s hands. I recall lots of fresh air, and being present in my body through discomfort and exhilarating exertion. There are many pleasant sensory memories: the smell of torn up field grass and dirt, the feeling of sunshine and cool New England air on our sweaty bodies, the taste of orange slices that we sucked on between plays, and the Gatorade that we drank from old coolers.
I also remembered the smell of mud which coated me from head to toe after I lost a bet with one of my teammates, and didn’t pay him in a timely manner. He was the captain of our team, and holds the ball in the photo above. He sent me flying face first into a deep and wide puddle. The bet was that I could score a goal on him during practice. I didn’t score the goal, and I couldn’t pay him right away. The result was one of the strongest memories of my childhood in which my mom refused to let my mud-covered self get into the car after practice and get muck all over her seats. She left without me, and I ended up running the distance between the practice fields and home, which was probably 3 to 4 miles. My dad came out to look for me in his car, and encountered me just a few blocks away from home. I don’t think I’ve ever run that far before or since in my life. I survived, but the experience cured me of any desire to make a wager with money on the line. (I did make an exception to this recently when I instigated a practice bet on Pierre’s microclot score).
I don’t think the parents were yet the “helicopter” type and mostly let the coaches do their job. Players didn’t get trophies simply for participating. I found it healthy to interact with other boys from different schools and I made a few friends.
I know that some of you will object to this assertion, but my experience has been that in life, most of us are losers. It’s not a radical statement. Anyone who watched the latest Super Bowl could sense the disappointment and pain of the losing team.
The patients for whom I have the least patience are the ones who continually ask “Why me? “ My first thought is, “Oh, you weren’t a loser like me.” My second thought is, “Why not you?” 5 billion people on this planet have been poisoned by the shots and the rest are being slowly poisoned by shedding. Come on team, let’s get it together, we’re all losers at some point. We can’t all be winners, and even winners can’t win every time.
Everybody loves a winner, but I think that having losing experiences as a child can prepare you mentally and emotionally for the world in which we live. Losers can still have a good life, and we do!
RECENT PAST
2014 was a big year for me. I graduated as a Family Nurse Practitioner from SUNY Upstate, started my first job as an FNP-C, and became the co-conspirator to lead a unionization drive in our local community hospital. There was a lot to lose, as we have lived in this town of Ithaca for twenty four years, and consider it our forever home. I’d worked at Cayuga Medical Center for fifteen years and had the respect and friendship of many. But, on the occasions when I made a med error in a busy Emergency Department, my own root cause analysis was that I had worked ten or more hours without a break. I reached my breaking point. I’d had enough and wanted to change our working conditions.
My partner in organizing was a spitfire ICU nurse named Ann Marshall. I love you Ann! We came from very different angles. I was a lifelong Democrat. She was a lifelong Republican. I’ve been a health nut for years and she was a closeted smoker. Wine was my thing, beer was hers. I was a vegan and she was a devoted carnivore. What we had in common was courage and integrity, with a bit of piss and vinegar for good measure.
Ann’s family had owned and run a steel mill in Connecticut. Because her family treated their employees well, providing safe working conditions and good compensation, they never faced a union drive. She was not a unionist by any stretch.
The maternal side of my family were Slovak immigrants who emerged from the coal mines of central Pennsylvania by opening an illegal saloon behind a storefront facade during prohibition. I joke that I come by my criminal tendencies naturally (E.g prescribing IVM during a pandemic). The saloon had a long oak bar that was broken up with axes by Federal agents. My Baba and Grandpop (first generation Irish, Duffy clan) opened a restaurant supply business outside of Philadelphia. No unions there.
It makes sense to me that the spark of a union began in the ED and the ICU, where you have the most independent thinkers and rabel rousers. The greatest opposition we had was from within the Maternal Child Health department, the OB/GYN nurses who had the best staffing, resources and working conditions.

Being new to unions, we didn’t think too long or hard about which union we chose to organize under, SEIU 1099. We, the organizing nurses, ended up running a guerilla campaign, raising our own funds and making some decisions which ended up angering the union leadership, while simultaneously drawing fire from the hospital management. For example, without the union’s permission, we paid for a billboard on one of the main roads into Ithaca, and ads on four Ithaca City buses.
The union leaders were furious that we had placed these ads without their permission, and that the billboard had the SEIU1099 logo on it. The hospital tried unsuccesfully to get the billboard taken down by threatening the ad company within two hours of placement. The hospital also tried to force the ads off the buses by marshalling their influence on the board of directors for TCAT, our city bus service. In a show of union strength and solidarity, the drivers and maintenance workers of United Auto Workers (UAW) Local 2300 told them to buzz off to the moon. If the board wanted to push the issue, there would be no buses running. In fact, we could only afford to pay for a month of ads but they stayed on the buses for more than four months. Thank you UAW!
The crucible of the union drive was stressful on all of us involved, as well as our families. Individual nurses such as Alicia and Erin took great risks to venture onto other units to try and get signatures for union cards. I hawked my dad’s college ring at the pawnshop to help pay for those ads. Nurses like Chicken Nugget (previously mentioned in Capital C Characters) overcame their fears and concerns for job security to continue meeting and organizing together. We truly believed that we were fighting for the safety of our patients as much as our dignity as workers.
Management for Cayuga Medical Center was ruthless and criminal—literally. The NLRB ultimately found them guilty of more than twenty violations of federal labor law. But in the end, they beat us. They had more money, time and lawyers, and kept appealing, and losing the NLRB decision, up through 2019. I was one of the first nurses to go in 2016, as the part-time schedule had fewer hours for me, and Ann wasn’t far behind me. Ultimately, out of a nursing staff of nearly 350, I think that more than 150 of us left. It’s fair to say that we were among the best and the brightest, and the most independent thinkers. It was not more than six months later that a patient died in the waiting room of Cayuga Medical Center from a treatable arrhythmia. The hospital pinned it on a travel nurse, but those of us who had been organizing knew better. It was precisely the outcome we were struggling to prevent.
PRESENT
This month marks the two year anniversary of our telemedicine practice, the Leading Edge Clinic. What started as the Dr Pierre Kory Advanced COVID-19 Care Center has evolved into a very experienced team which is nurse-driven, patient-focused and provides compassionate care for complex conditions. Having cut my teeth in the business world and written ad copy for a small business, I realize that those words may sound like pap. The truth is that they are based upon what we actually do, who we really are, and what keeps us showing up for our patients.
Why nurse driven? In most healthcare settings, nurses barely reach the potential of their scope of practice. In our practice, the nurses have accumulated a great deal of expertise in the treatment of post-acute sequelae of COVID (PASC), and COVID vaccine injury. In order to meet the intense needs of our complex patients, the nursing team spends an exceptional amount of time with them. It never feels like enough, it stretches our budget, and yet it far exceeds the quality and duration of what most people have experienced in a lifetime of interactions with our broken healthcare system. We are also a nurse-driven team, because as the managing partner of this practice, I am a nurse first and foremost, and I am proud of the history of nurses focusing on the whole person, and promoting health, in a way that I have always found distinctive from the medical school disease-focused model which moulds the physician. Growing from the RN role into the FNP role, I have relished and embraced the many opportunities for patient education. It is what RNs and Nurse Practioners do best! Finally, we are a nurse driven practice because the single physician in our midst is a humble and decent human being, a man whose head hasn’t swelled with his renown, and who recognizes and depends upon the skillful and intelligent nursing team which drives our care.
Historically, I usually find out that I’ll be joining Pierre in some sort of discussion at the last minute. It’s usually a text that says “you and I are going to appear on _____ at _____ (time).” It’s probably just as well that that’s how it goes because it leaves me little time to object or decline. That’s how it went at the FLCCC conference when I ended up on stage with Dr. Marik and Pierre doing case reviews. If you’ve watched their repartee, it’s kind of like being the odd man out in an Abbott and Costello routine. My apologies to the younger people who are reading. Abbott and Costello were two famous comedians from the black-and-white movie era.
What struck me most as we were listening to those three case reviews was that ivermectin was not front and center on a daily basis in any of them. This is something that I don’t quite understand. The FLCCC Alliance has made a Herculean effort to educate providers and patients alike about the central role of ivermectin in preventing Covid, treating acute Covid, as well as treating long-haul and vaccine injury. Yet these patients were not receiving it. Pierre even wrote a book on the subject.
In part it is for this reason that I thought it worth your time, and my time to make the case for daily use of ivermectin from this point forward. Starting with the basics. Ivermectin is one of the safest medication‘s known to humankind. In the context of Covid we understand that it neutralizes spike protein, decreases inflammation, modulates immune response, and stabilizes mast cells. Even if you don’t have PASC or vaccine injury, but you believe shedding is real, those are all good reasons to keep on taking ivermectin on a daily basis.
But wait, there’s more! Ivermectin is showing itself to be invaluable in preventing and treating cancer. It made it onto the list of repurposed therapeutics that Dr. Marik and the FLCCC Alliance listed in his monograph on cancer treatment. It will play a central role in the protocols used by the five practices participating in the FLCCC Alliance cancer study, one of those practices being ours. However, the single most important reason why I advocate that my patients continue to take ivermectin on a daily basis, is the role that it plays in relation to micro clotting.
We all have our heroes from this pandemic. Although it makes me shudder, I realize that for some people that hero is Dr. Fauci. One of my heroes is a man whose name you may not have heard of, but who has profoundly influenced my clinical practice. He is Dr David Scheim, a semiretired officer of the United States Public Health Service Commissioned Corps. In February 2022 he published a theoretical paper about the role of ivermectin in relation to red blood cells and platelets. He posited that because of its effect on CD 147 receptors on the surface of red blood cells (RBCs) and platelets, ivermectin prevented the spike protein from triggering platelet activation and aggregation, and red blood cell (RBC) aggregation, or a agglutination. He also put forward some calculations about the number of molecules of ivermectin in proportion to RBCs could be expected when doses of 0.2 mg per kilogram were delivered. “For a dose of IVM administered with food in the standard, non-aggressive range of 200–350 µg/kg, the peak plasma level (at +4 h) of IVM plus active metabolites would be approximately 412 nM, which amounts to 52,000 molecules of IVM and active metabolites per RBC in human blood.” The numbers were very reassuring. (My editor told me to translate the above in lay terms. Essentially, with low doses of IVM, there is an enormous amount of IVM in proportion to the cells in our body which can form abnormal and harmful microclots.)
That relatively brief paper, that clinical hypothesis, and those numbers, gave me the confidence to continue swinging away with ivermectin over the last two years with thousands of patients. When I encountered colleagues who hold up treating the Microbiome as the be-all-end-all of clinical care, I can listen to what they say, but hold on to what I think is a more important truth. The microbiome can be healed over time, but coagulopathy can kill you now.
In the Winter of 2022 Dr Scheim et. al. published another paper titled SARS-CoV-2 Spike Protein Induces Hemagglutination: Implications for COVID-19 Morbidities and Therapeutics and for Vaccine Adverse Effects. Then in the Fall of 2023 Dr. Scheim et. al. published a « piece de résistance » regarding ivermectin and the role that it plays in relation to endothelial cells, red blood cells, and platelets. Dr. Marik kindly shared it with the understated subject line “cool paper. “ One of the most important assertions of this paper is a statement of fact, that individual endothelial cells have 38,000 glycan receptors and only 175 ACE2 receptors. Additionally, platelets and red blood cells have zero ACE2 receptors, but are covered with glycan receptors. Given the profound impact of the spike protein, following injection, entry into the bloodstream, systemic endothelial injury, and provocation of clotting, the dearth of ACE2 receptors in that initial pass has enormous significance. In both the popular press, and the circles of practitioners treating PASC and vax injury, the conversation has been dominated by the narrative that the ACE2 receptor is the penultimate target of the spike protein. What if we expand our understanding to include glycan receptors?
Dr. Scheim et. al. elucidate in great detail how profoundly ivermectin protects endothelial cells, RBCs, and platelets from the harm of spike protein, additionally contributing to the resolution of injury and coagulopathy. By both expanding the narrative beyond ACE2, and explaining the profound clinical action of ivermectin on the blood vessels, and in the bloodstream, Dr. Scheim et. al. help propel ivermectin into the Covid Hall of Fame for years to come. Retrospectively, their research vindicates the brave practitioners who dared to prescribe ivermectin to their patients in the face of blistering criticism and specious slander.
Having been a loser for so long, I’m accustomed to ongoing struggle. I think that we have lost the war of this pandemic, and are fighting skirmishes to save the lives of as many people as we can. Ivermectin has been and continues to be a reliable and versatile tool in our fight. After two years working together, I can say that whatever the future may hold, whatever the final outcome of this historic battle for humanity, the good people of The Leading Edge Clinic have formed a winning team.
P.S. Thanks to Beck for his song Loser, and Randy Travis for his song Better Class of Losers for their musical inspiraiton while writing this Substack.
See previous comment. At this point it should be possible to get human tabs from India if you don’t have a prescriber.
In general, 12mg appears to be an adequate dose for maintenance, but it really depends on the individual’s circumstances.