
Case Study: Longitudinal Analysis of Neurotransmitter Profile Changes in Post-COVID Syndrome
Insights from the ZRT urine neurotransmitter test




Patient Background
This patient of the Leading Edge Clinic is a middle-aged female with a history of post-COVID syndrome following vaccination (two mRNA Pfizer doses, last administered 4/22/21) and COVID-19 infection (onset 12/16/22). Her medical history includes cystic acne, GERD, and menstrual irregularities. She has experienced anxiety, sleep disturbances, and fatigue as part of her post-COVID symptoms. The patient has undergone multiple therapeutic interventions, including NAC Augmentata, Memantine, HBOT sessions, and nutritional supplementation including 5-HTP.
Discerning whether a patient’s constellation of symptoms reflects post-acute sequelae of Covid (PASC) or injury from the Covid shots is an imprecise art. In the case of this patient, I would argue that there are two factors which argue towards vaccine injury, and one which argues against. The first is that both of her Pfizer shots were from bad batches.
https://www.howbadismybatch.com
Pfizer
BATCH ADRs DEATHS DISABILITIES LIFE THREATENING ILLNESSES
ER8734 1944 15 31 39
EW0169 1589 15 26 20
The second factor is that her initial spike antibody, as measured by the Lab Corp IgG test was >25,000 U/mL.
Date Collected: 2/19/2024 Ordered Items:SARS-CoV-2 Semi-Quant Spike Ab A, 01 See Dilution: >25,000 U/mL, Positive
(Negative<0.8)
Exceeding the top of the scale, this patient’s levels reflect a massive immune response to the shots. We tracked her spike ab level, and over time, in response to therapies which detach spike protein from cell receptors, and break down it down, we saw her level drop to 15,780 U/mL by October of 2024.
The third factor which argues against vaccine injury is that there wasn’t temporal association between vaccination and onset of symptoms. I.e. symptoms didn’t start after the first Pfizer, or the second Pfizer in April of 2021. It wasn’t until October of 2022 that things got messy. But, that was more than two months before her first known infection with Covid. What happened in October argues towards vaccine injury, because something which used to be a rare occurrence increased by 2000% during the months following the rollout of the Covid shots: decidual cast shedding. From my note:
We discussed the pathology of spike protein penetrating ovaries causing hormone dysregulation and decidual cast shedding. Reports last month she experienced passing a “large clot that was larger than anything I have seen since giving childbirth." We discussed how during perimenopause anovulatory cycles occur, progesterone being low, causing an increase in endometrial lining , heavy menses, anxiety and insomnia. Consider hormone balance if symptoms are not relieved with current plan.
Initial Neurotransmitter Testing (September 2024)


A comprehensive ZRT urine neurotransmitter panel was conducted on 09/04/24, revealing significant imbalances in multiple neurotransmitter systems. Initial testing showed 13 of 27 measured neurotransmitters were outside the optimal range1.
Key findings from the initial test included:
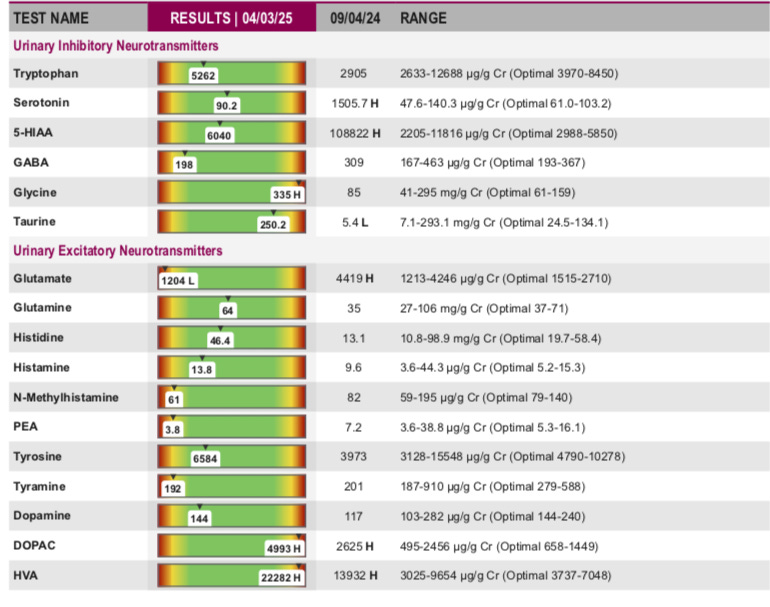
Serotonin pathway abnormalities: Low-normal tryptophan (2905 μg/g Cr; optimal 3970-8450), elevated serotonin (1505.7 μg/g Cr; optimal 61.0-103.2), and elevated 5-HIAA (10822 μg/g Cr; optimal 2988-5850).
Catecholamine deficiencies: Low-normal norepinephrine (10.2 μg/g Cr; optimal 15.0-28.1), normetanephrine (17.6 μg/g Cr; optimal 17.9-31.7), and epinephrine (1.2 μg/g Cr; optimal 1.4-4.2).
Excitatory neurotransmitter imbalances: Elevated glutamate (4419 μg/g Cr; optimal 1515-2710), low-normal glutamine (35 mg/g Cr; optimal 37-71), and low-normal histidine (13.1 mg/g Cr; optimal 19.7-58.4).
Inflammatory pathway markers: Kynurenine (276 μg/g Cr; optimal 257-960) and low-normal 3-hydroxykynurenine (134 μg/g Cr; optimal 147-467).
Dopamine system dysregulation: Low-normal dopamine (117 μg/g Cr; optimal 144-240) with elevated DOPAC (2625 μg/g Cr; optimal 658-1449) and elevated HVA (1392 μg/g Cr; optimal 3737-7048).
Other notable findings: Low taurine (5.4 L mg/g Cr; optimal 24.5-134.1), normal GABA (309 μg/g Cr; optimal 193-367), and elevated NorEpi/Epi ratio (8.5; optimal 5.2-13.7).
These findings were interpreted as evidence of severe adrenal fatigue, glutamate excitotoxicity, and metabolic disturbances consistent with ongoing inflammation and neurological effects of spike protein.
Therapeutic Interventions
Based on the initial results, the following interventions were recommended and implemented:
Discontinuation of 5-HTP supplementation
Addition of Lithium orotate 5mg daily
Bacopa 500mg twice daily
Vitamin D3 30,000 IU daily
Extended-release Memantine 7.5mg daily
Dr. Wilson's Adrenal Support supplements
Black Currant Gemmotherapy
Phyto curcumin supplementation
Follow-up Visit One Month Later
Patient reports getting up at least a few times in the night to void. Some days around 3pm she gets a little tired. Engaging in weight-lifting and walking. Tries to do heavier weights, and walking about 1 1/2 miles nightly as a family. Using NIR sauna about 3-4x/week for about 25 minutes. Appetite is good, without limitations to what she can eat, good GI function. Libido is lower, cycles occurring less often. A few months ago it was two weeks late, the next month a week early, then didn’t have one, and one showed up randomly. Baseline amyloid fibrin microclotting measured at stage/grade 2 of 4, mild.
Updated Treatment Plan
Based on the follow-up visit, the treatment plan was modified:
Continued adrenal support with focus on catecholamine precursors
Sulodexide 250 LSU (25mg) daily for anticoagulation, endothelial repair
Gradual weaning from L-Lysine, Moomiyo (Shilajit), and 5-HTP
Discontinuation of protein powder due to autophagy inhibition
NIR sauna therapy (Optimized at 10 minutes once or twice daily for mitochondrial function instead of 25 minutes)
Continued weight-bearing exercise and walking to stimulate long-bones to produce stem cells
A follow-up ZRT urine neurotransmitter panel conducted on 04/03/25 revealed several significant changes:

Improvements:
Norepinephrine: Increased from 10.2 to 12.1 μg/g Cr (still below optimal range of 15.0-28.1)
NorEpi/Epi ratio: Improved from 8.5 to 12.1 (optimal 5.2-13.7)
3-Hydroxykynurenine: Increased from 134 to 383 μg/g Cr (now within optimal range of 147-467)
Creatinine: Improved from 0.29 L to 0.49 (still below normal range)
VMA: Decreased from 4436 to 4195 μg/g Cr (approaching normal range)
Persistent abnormalities:
Kynurenine: Increased from 276 to 516 μg/g Cr (now within optimal range of 257-960)
Kynurenic Acid: Decreased from 1048 to 772 μg/g Cr (still within normal range)
Xanthurenic Acid: Decreased from 1325 to 1090 μg/g Cr (still within normal range but improved)
Epinephrine: Decreased from 1.2 to 1.0 μg/g Cr (further below optimal range of 1.4-4.2)
Normetanephrine: Decreased from 17.6 to 16.3 μg/g Cr (now below optimal range of 17.9-31.7)
Clinical Correlation
The longitudinal comparison of neurotransmitter profiles reveals a mixed pattern of improvement and ongoing dysregulation. The most notable improvements occurred in inflammatory markers and certain catecholamine metabolites, suggesting a reduction in neuroinflammation and partial recovery of autonomic nervous system function.
The patient reported some clinical improvement in daytime energy levels but continued to experience nocturia, afternoon fatigue, and ongoing menstrual irregularities1. The persistent low catecholamine levels (norepinephrine and epinephrine) correlate with her reported afternoon fatigue and likely reflect ongoing adrenal dysfunction despite treatment.
Improvements in the kynurenine pathway markers suggest reduced neuroinflammation, which may explain the patient's subjective improvement in cognitive function and reduced anxiety. The NorEpi/Epi ratio improvement indicates a better balance between sympathetic and parasympathetic nervous system activity, though the absolute values of these neurotransmitters remain suboptimal.
Discussion
This case illustrates the complex neuroendocrine disruptions that can persist in post-COVID syndrome. The initial neurotransmitter pattern showed features consistent with:
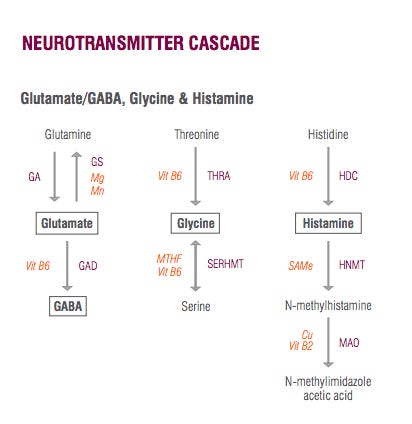
Excitotoxicity: Elevated glutamate and altered glutamate/GABA balance
Serotonin dysregulation: Low tryptophan with paradoxically elevated serotonin and 5-HIAA
Catecholamine deficiency: Low norepinephrine, normetanephrine, and epinephrine
Inflammatory activation: Altered kynurenine pathway metabolites
The follow-up testing seven months later showed partial normalization of several parameters, particularly in the inflammatory pathway, suggesting that the targeted interventions provided some benefit. However, persistent abnormalities in the catecholamine system indicate ongoing dysregulation of the stress response system and adrenal function.
The ZRT urine neurotransmitter test has been used by this practitioner with more than seventy patients over the last two years. This patient is one of four who chose to repeat the study, providing an opportunity to study and better understand the measurable results of interventions, and correlate them to the patient’s trajectory of recovery. The cost of this test, ranges from $235 (what we charge for the test and clinician interpretation at the Leading Edge Clinic) to $330 from different sources. We order the test through Rupa Labs, the kit is mailed to the patient, and she/he provides four urine and one saliva specimen. There is a questionnaire to complete, and if the patient provides information about supplements and Rx medications, it helps with the test interpretation. E.g. in the repeat neurotransmitter test for this patient, elevated DOPAC and HVA could be correlated with the use of bioflavanoids such as quercetin, and this is a supplement which she has listed on her most recent records.
Conclusion
This case study demonstrates the utility of comprehensive neurotransmitter testing in guiding targeted interventions for post-COVID syndrome. The longitudinal comparison revealed partial improvement in neurotransmitter balance over a seven-month period, correlating with modest clinical improvement.
The persistent abnormalities, particularly in the catecholamine system, suggest that neuroendocrine recovery from COVID-related damage may require extended treatment and monitoring. This case highlights the importance of personalized, biochemically-guided approaches to treating complex post-viral syndromes, vaccine injury, and the value of sequential testing to assess treatment efficacy and guide ongoing intervention strategies.
That neurotransmitter test looks pretty interesting. Maybe I should get one!
Whenever I hear about low tryptophan issues, I think "pellagra" (intracellular, or systemic), based on studies done 25 years ago. Something (maybe that inflammation) is sucking up all the NAD, which if niacin is insufficient, ends up grabbing the tryptophan (60:1 conversion rate) because NAD is just that important. And the downstream stuff from tryptophan no longer gets produced (serotonin, melatonin).
So the cascade is: low NAD => low TRP => low SRT/MLT => no sleep, not happy. And "brain fog" (pellagra #3: dementia) too.
The study showed that the "pellagra" dropped when cells (and later, patients) were treated with high dose niacinamide.
A NAD precursor might be a band-aid for the tryptophan issue, but getting rid of that underlying cause of inflammation seems best. Interesting how this outcome shows up in that test.
I asked about a friend today who had "long covid". He told me she now has dementia! Is there a connection??