
From Fatigue to Fertility: Spring 2026 Update
Continued Mercury Mobilization in Viable Late-Pregnancy


An observational clinical account from my practice as Scott Marsland, FNP-C at Leading Edge Clinic
In November 2025 I published the initial case study of a woman whose chronic fatigue and long-standing infertility shifted dramatically after targeted mineral repletion with a liquid volcanic mineral solution chemically similar to EPA-approved water purification formulations such as Aurmina. I updated this case study in March of 2026. The pregnancy remains fully viable with an expected delivery in July 2026. The patient continues to be healthy and active overall, with only expected pregnancy-related fatigue.
Patient Update (May 2026)
The patient shared the following:
Continuing 5 mL oral twice daily (morning and evening) in treated water.
Walking one hour daily and practicing yoga every day.
Feeling tired, which she attributes to pregnancy, warmer weather, recent extensive travel, and periods of less optimal water/food access. She also wonders about prior Celtic salt use.
No recent bathing, but consistently using the treated mineral water for drinking, tea, coffee, and cooking.
Recent midwife blood work: no urinary protein (reassuring for renal health), low ferritin with high serum iron. She suspects insufficient vitamin C co-administration with her iron supplement affecting conversion/storage; she is addressing this.
Fetal monitoring via Doppler shows strong heartbeat and active movement (kicking). Formal ultrasound scheduled at 34 weeks.
Lab Timeline & Key Changes (April 20, 2026 Results)
Figure 1: Mercury Speciation (Quicksilver Scientific)
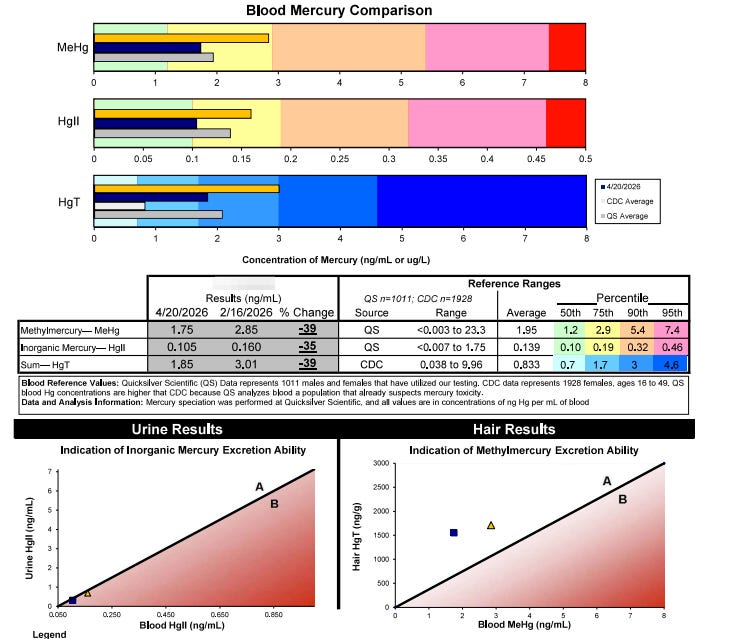
Figure 2. Summary of Mercury Changes Over Time

Overall from baseline (June 2025): MeHg –79%, Total Hg –78%.
Urine mercury indicates strong excretion capacity (total Hg –54% from prior). Hair mercury at 1,550 ng/g consistent with ongoing mobilization.
Whole-Blood Elemental Panel (April 20, 2026)
Figure 3: Nutrient + Toxic Elements
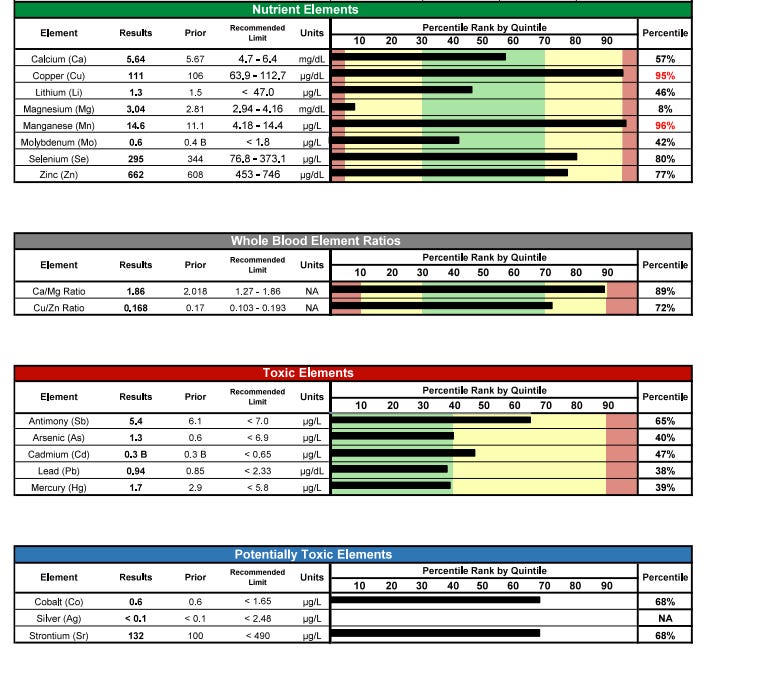
Notable trends:
Mercury continued declining to 1.7 µg/L
Zinc improved to 662 µg/dL (77th percentile)
Magnesium improved to 3.04 mg/dL
Selenium stable at 295 µg/L (80th percentile)
Lead stable/low; other toxics well-controlled
Discussion
Despite recent travel and reduced bathing, the patient’s consistent oral intake and use of treated water for daily cooking/drinking appear sufficient to sustain impressive mercury reduction (–39% since February, –79% overall for MeHg). The low ferritin/high iron pattern is common in pregnancy and is being addressed with added vitamin C. Fetal status remains reassuring.
These patterns continue to align with the mineral displacement, selenium-supported demethylation, and enhanced clearance mechanisms explored in Dr. Pierre Kory’s water chemistry framework.
The temporal association between sustained mineral support, heavy-metal mobilization, and a healthy ongoing pregnancy remains striking. The patient’s tolerance and continued progress speak to the protocol’s gentleness and adaptability even under the physiologic demands of late pregnancy and travel.
Disclaimers
Aurmina is an EPA-approved water purifier only and is not a supplement or drug. This is a single observational case. It is not intended to diagnose, treat, cure, or prevent any disease.
Next Steps
Third-trimester labs, 34-week ultrasound, and postpartum retesting at 6–8 weeks (once plasma volume normalizes) to assess sustained improvements.
Thank you for reading. I welcome thoughtful questions in the comments.
Scott Marsland, FNP-C
Lightning Bug | Leading Edge Clinic
Come for the science, stay for the stories.
Personal reflections (including the My Vietnam series, Part 1, Part 2, and Part 3) live in the opt-in Personal Insights section—toggle it on in your account settings if they speak to you.
I think that if you go back to the first presentation I made at an FLCCC conference you’ll see that I was an early adopter and advocate of using spike antibody testing to help guide clinical diagnosis and treatment. Today you’ll see some of the most prominent and respected medical professionals in the PASC and Covid vaccine injury space loudly proclaiming that spike ab is the test to get and will serve both patient and clinician in clinical treatment.
After more than four years of practice in the space and studying the results for thousands of our patients, I could not disagree more. There is some very limited value to getting spike antibody levels. There is much more value to directly measuring qualitatively and quantitatively the levels of spike and spike fragments in monocytes, endothelium, exosomes and commensal bacteria of the G.I. tract. That technology already exists, has been approved by European regulatory agencies, and both European and American companies are racing to bring it to market. Once that testing is in place and validated, I don’t think boo will be said about spike, antibody levels anymore.
I haven’t seen this tested in an infant, and frankly wouldn’t bother. Better testing is on the way.
Hi Scott, just a general question not specific to this case but wondering if any of your patients at the clinic or elsewhere have done a spike protein antibody test on a newborn baby to check and see if the baby has spike protein if mom to be or dad to be was exposed to covid during the pregnancy or even if mom was vaccinated back in 2020 or 2021. Any stats or recommendations?